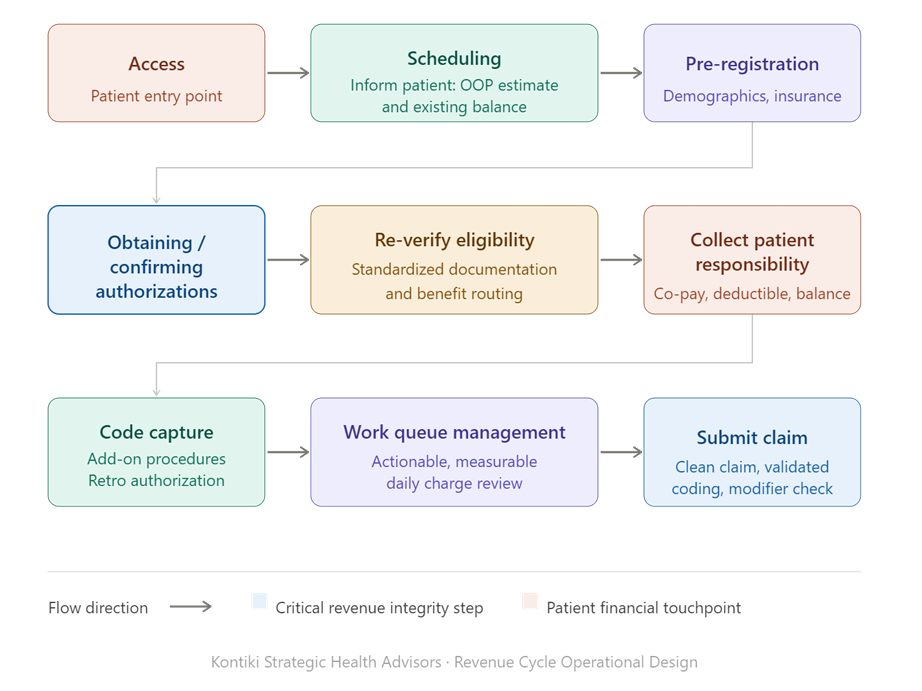
The revenue cycle begins with accurate patient access, including scheduling, registration, eligibility verification, and authorization, followed by precise clinical documentation, charge capture, and compliant coding to support clean claim submission. Claims must be submitted in a timely and accurate manner to ensure payer adjudication without delay. Any denials, edits, or missing information must be actively managed through structured work queues and rapid resolution processes to prevent revenue leakage. The objective is consistent achievement of gross collections from both payor reimbursement and patient responsibility, net of contractual adjustments, through disciplined, end-to-end operational execution.
“Sustainable performance improvement requires transparency. While outcomes are embraced, the process often surfaces gaps and errors that can create discomfort. That is where real progress occurs. When approached collaboratively, those insights become catalysts for stronger execution, better outcomes, and a more aligned, high-performing team. In this environment, measurable data is the ultimate source of truth.”
Michele Kadlec
Chicago, Illinois 2022
An example of scaling operations across multiple locations was during my work leading enterprise performance improvement across a multi-site medical group and CIN structure, where I was responsible for aligning operations, revenue cycle, and value-based performance across primary care, specialty practices, and ancillary services.
At the time, the organization was highly fragmented. Each location operated with different workflows, inconsistent front-end processes, variable coding practices, and limited visibility into financial performance. This resulted in missed charges, high denial rates, leakage across service lines, and inconsistent patient access.
The key challenges fell into three areas:
- First, lack of standardization. There were no consistent workflows from pre-registration through charge capture and collections, which created variability in both patient experience and financial outcomes.
- Second, limited data transparency. Leadership and practice managers lacked access to actionable, real-time metrics at the location- or provider-level, making it difficult to drive accountability.
- Third, misalignment between operations and value-based care. Activities such as Annual Wellness Visits, RAF capture, and transitional care management were not being executed consistently, leaving both revenue and quality performance on the table.
My approach was structured and scalable: I implemented what I call a “two bookends” operating model, anchoring every location between access and scheduling on the front end and confirming gross collections net of contractual adjustment on the back end. Between those bookends, we standardized workflows across all sites, including real-time eligibility, authorization integrity, charge capture, coding accuracy, and denial management.
We created a service line–based governance model with clear accountability at each level: front-end staff, RCM, coding, and physician leadership. This ensured that every location operated under the same expectations, while still allowing for specialty-specific nuances.
From a data standpoint, I partnered with analytics teams to deploy enterprise dashboards that tracked KPIs such as charge lag, denial rates, work queue volumes, wRVU-to-collections ratios, and referral leakage. These were rolled out consistently across all locations, enabling transparent performance management.
To support value-based care scaling, we embedded workflows for AWVs paired with problem-oriented visits, improved MEAT documentation for RAF accuracy, and integrated TCM and care gap closure processes directly into practice operations. This allowed us to improve both fee-for-service revenue and value-based performance simultaneously.
We also focused heavily on training and change management. I took a “boots on the ground” approach, working directly with practice managers, physicians, and staff to reinforce workflows, close gaps, and ensure adoption. Every change was tied to measurable outcomes and reinforced through ongoing performance reviews. Sustainable performance improvement requires transparency. While outcomes are embraced, the process often surfaces gaps and errors that can create discomfort. That is where real progress occurs. When approached collaboratively, those insights become catalysts for stronger execution, better outcomes, and a more aligned, high-performing team. In this environment, measurable data is the ultimate source of truth.
The results were both measurable and sustainable. We significantly reduced charge lag and denial rates, improved first-pass through claim acceptance, increased net collections, and reduced outmigration by strengthening internal referral pathways. At the same time, we improved RAF capture and quality metrics, which supported long-term value-based contract performance.
What made this successful was not just implementing change, but building a scalable operating framework that could be replicated across locations, service lines, and markets while maintaining accountability and financial discipline.